

If anything has defined my current dedication to knee injuries, it has undoubtedly been having mentors. Professionals who opened doors for me and allowed me to make the most of my curiosity. One of them was the Dutch physiotherapist Nicky van Melick, author of the most recent scientifically published clinical practice guideline for anterior cruciate ligament (ACL) rehabilitation. Shortly after its publication, Nicky came to Spain to deliver a course that I attended, where I also had the opportunity to meet her personally and receive her invitation to undertake a short clinical observership with her in Eindhoven.
We remained in close contact from then on, but it was not until the 2024 Isokinetic Conference held in Madrid that we had the chance to meet again. Nicky attended as a speaker in the oral communications sessions to present her latest research in the psychosocial domain of ACL injuries, and I—having the opportunity that year to attend one of the most internationally relevant conferences practically at home—was not about to miss it, nor the chance to spend time reconnecting and meeting new colleagues.
The Isokinetic Conference was undoubtedly filled with highly interesting talks and debates on ACL injuries, addressing the most current and challenging topics facing both the clinical and scientific communities. But it was also filled with hours outside the conference, sightseeing around Madrid or sharing beers in a bar. And it was during one of those rounds, seated on the terrace of the Irish Rover, that I said to Nicky, “Hey, could I ask you a few work-related questions?” Because I can certainly imagine what it’s like to have people constantly talking to you about knees 🙂. After she agreed, I pulled a notebook and pen out of my backpack so as not to waste a second and asked my first question—one I had been genuinely curious to pose:
“Nicky, the guideline was published in 2016, and almost 10 years have passed.
What would you change, and what would you include if you were to redo it today?”

As you can imagine, the conversation went on for quite some time. Whenever I explain this guideline in training courses, I always insist on one idea: that, in my view, many things are missing from it, and therefore my goal is not for physiotherapists to learn it by rote, but to understand that it is a guideline—what a phase is, how objectives are set, which functional criteria should be assessed, and so on—so that they are able to interpret any guideline they may have in front of them and, above all, become autonomous in developing their own professional evolution. Many clinicians have been calling for an update, myself included.
I gathered everything we discussed into a list and, at the end of the conversation, I mentioned to Nicky the idea of writing an article about it on the Knee Spain blog, so that it wouldn’t remain just between the two of us and could be shared with anyone interested. Her answer, however, was no: “because I’m going to do something better—an editorial article.”
After the summer, Nicky wrote to me asking for the transcription of the notes I had kept from that conversation, and in February 2025, this article was published:

So now yes, this is the moment when we both decided to write this blog post about the content of that editorial and, in doing so, discuss it with all the professionals within the knee community who wish to take part.
AG: Work on this guideline began in 2014 and it was published in 2016. What was the context like at that time in the field of ACL injuries? What was the situation, and what motivated its development?
NVM: In fact, everything started in 2012 with the development of a Dutch ACL rehabilitation guideline, commissioned by the Royal Dutch Society for Physical Therapy. At that time, there was no specific guideline in the Netherlands for patients undergoing ACL reconstruction.
I had just started my PhD on ACL rehabilitation, and I was asked to be the first author of this guideline. From the very beginning, I knew it was a project that would have a major impact. To put it into context, the center where I worked as a physiotherapist and researcher was one of the few places where patients were assessed using strength and hop tests, something that was not common practice in 2014.
When the Dutch guideline was completed in January 2014, the rest of the working group and I felt that we had developed a project that was relevant enough to share with the rest of the world. That is why we decided to write an article in English for the British Journal of Sports Medicine.
AG: And what impact did that article have? What kind of feedback did you receive in the years that followed?
NVM: I feel that this marked the beginning of my international career. Suddenly, many people knew my name and started reading my papers.
I remember that in 2020, for a presentation related to my doctoral thesis, I asked BJSM for information about all the countries in which my guideline article had been downloaded, and I created a map using those data. It was incredible to see. It is a curious experience when people “know you” and start sending you emails or messages on social media with questions about ACL rehabilitation. All of a sudden, I became a reference in this field. I always tried to respond to all of those questions.

AG: So, starting with the main question from that afternoon, almost 10 years have passed since the publication of the ACL clinical practice guideline and, during this time, research has continued to provide us with more information. In your opinion, what would be the main aspects you would include now that were overlooked in the original guideline?
NVM: Mainly three.
- OKC: Many things were published afterward.
- Neurocognitive domain: Nowadays, we are told that this is a very important component and that it should be addressed from the very beginning. Our review only mentioned one study that did not demonstrate effectiveness, and it was therefore not directly included in the guideline.
- Psychosocial factors: These were not mentioned in the review and only appeared in the guideline through PROMs within the recommended assessments.
AG: Let’s then talk more specifically about each of these points, starting with OKC exercise prescription.
In your guidelines, you proposed not introducing OKC exercises until week 4 for BPTB grafts and until week 12 for hamstring tendon grafts. Other guidelines also supported not introducing them before week 4 (Adams 2012, Wright 2015, van Grinsven 2010, Kotsifaki 2020) and starting with a restricted range of motion from 90° to 45°. These recommendations were based on the limited evidence available at the time regarding this topic in patients undergoing ACL reconstruction.
It was in 2020 that this debate was reignited with the popular article by Noehren and Snyder-Merkle in JOSPT, titled “Who’s Afraid of the Big Bad Wolf?”, following a study published that same year by Eglander. This study reported, using 3D MRI models in a sample of ten healthy subjects, that ACL strain was 12% during the heel strike phase and 5% during mid-stance.
When comparing this study with another highly cited paper in the field by Escamilla (2012), which reported a strain of 4.4% during isometric contraction at 15° of knee flexion with 80–100% load, also in healthy subjects, this group decided to introduce OKC exercises immediately in their guideline published in 2022 (Brinlee 2022).
However, it was Forelli’s research in 2023 and 2024, after decades of articles that focused mainly on functional criteria, that provided clearer evidence.
In 2023, Forelli published a study in postoperative patients in which no changes in graft laxity were observed. In this study, exercises were performed exclusively in CKC (closed kinetic chain) in the control group, and in CKC combined with loaded OKC from week 4 onward in the experimental group, always meeting functional criteria such as a stroke test score of less than 1, a minimum range of motion of 0°–110°, and the ability to perform a straight leg raise without an extension deficit. All patients had hamstring tendon grafts, and the experimental group showed better strength symmetry values at 3 and 6 months, with no differences in laxity compared with the control group.

In 2024, the same groups were compared again, this time introducing OKC without resistance in week 2 and with resistance in week 4, obtaining similar results.
Therefore, introducing OKC exercises from week 4 onward appears to be safe, even in patients with hamstring tendon grafts. In addition, we know that before this time point, beyond biological criteria, functional factors such as effusion, pain, or limited mobility prevent most patients from being able to perform this type of exercise.
Now that you are fully dedicated to research, but based on these reflections, if you were to return to clinical practice, with the current level of evidence and the experience from your most recent collaborative projects, what progression would you follow to introduce OKC exercises in a patient with a hamstring tendon graft? And in a patient with a BPTB graft?
NVM: Once effusion and pain are under control.
Before starting OKC exercises on a machine, quadriceps activation can be initiated without any added resistance, for example, with OKC isometric exercises against a ball, or by working the last 30 degrees of knee extension while seated on a plinth with a small roll placed under the knee. But again, it is essential to pay close attention to the knee’s response.
The first priority is to ensure that, when starting OKC exercises on a machine, the knee is calm. That is, minimal effusion (trace or 1+ on the stroke test), full extension at 0°, and a normal gait pattern.
At that point, it is possible to introduce OKC quadriceps strengthening exercises, for example, on a knee extension machine with a full range of motion. I would always start with low resistance and then assess the knee’s response afterward. If there is an increase in effusion, pain, or stiffness, the exercise is probably too demanding and it would be advisable to wait.
With current surgical techniques, I do not consider there to be significant differences between autograft types.
AG: And one final question regarding OKC exercises. In your most recent article, you mention that “OKC quadriceps exercises may be less functional.” My question is, can functionality be trained without first addressing analytical deficits?
NVM: OKC exercises are less functional, but they are necessary to specifically target the knee extensors. With more functional exercises, such as squats, there is always the possibility of compensating with, for example, the hip extensors, which could result in a lack of strength gains in the quadriceps.
Therefore, I believe the best option is to combine less functional but more isolated exercises with more functional ones.
AG: Perfect. With OKC exercise prescription clarified, let’s move on to the neurocognitive domain. We know that knee joint injuries are not only biomechanical, but also neurological, affecting proprioceptive function. This alters the sensory system, producing changes at the brain level as well, and this aspect is being discussed more and more. However, when you wrote your guideline, you only mentioned the study by Caprelli on this topic, which concluded that exercise prescription in this domain had no effect.
It was between 2015 and 2017 that Grooms began to highlight the importance of addressing both hardware and software, explaining the nervous system adaptations following ACL injuries. However, the review published by the Aspetar group (Kotsifaki 2024) also does not include this domain, beyond again mentioning the Caprelli study.
Authors such as Gokeler, Chaput, and Lepley have discussed this process of neurological waiting, emphasizing the cognitive factors that influence how information is gathered, processed, and responded to, and introducing concepts such as visual dominance, reaction time, motor learning principles, dual-tasking, and external focus. And this applies not only to treatment, but also to assessment. In the last two editions of the Isokinetic Conference in Madrid, this neurocognitive topic has had major relevance, being discussed in several panels composed of researchers.

AG: Nicky, in your article “Decades of Change”, you mention that many physiotherapists need to change their way of thinking regarding the neurocognitive domain in order to close the gap between research and clinical practice. However, the guidelines themselves do not address this topic from the outset. Why do you think that, despite this growing body of research, contributions related to the nervous system are still not included?
NVM: The main reason with the Aspetar guideline is that they only included randomized controlled trials (RCTs). And since there are no RCTs comparing neurocognitive training versus no neurocognitive training, it was not included in their guideline.
In our guideline, we only included articles published up to June 2015. In addition to RCTs, we also included prospective studies. But, to my knowledge, there were no prospective studies describing neurocognitive rehabilitation in a patient sample.
Once this topic is included, I personally believe that the first challenge would not be incorporating it into our treatments, something that perhaps a small percentage of physiotherapists already do in their daily practice, mainly those who are more knee-focused.
AG: Yes, and perhaps the real challenge would be incorporating it into our assessments. This is where, as a clinician, I feel there is a major gap between research and practice. Nicky, what cognitive measures are suggested in the scientific literature?
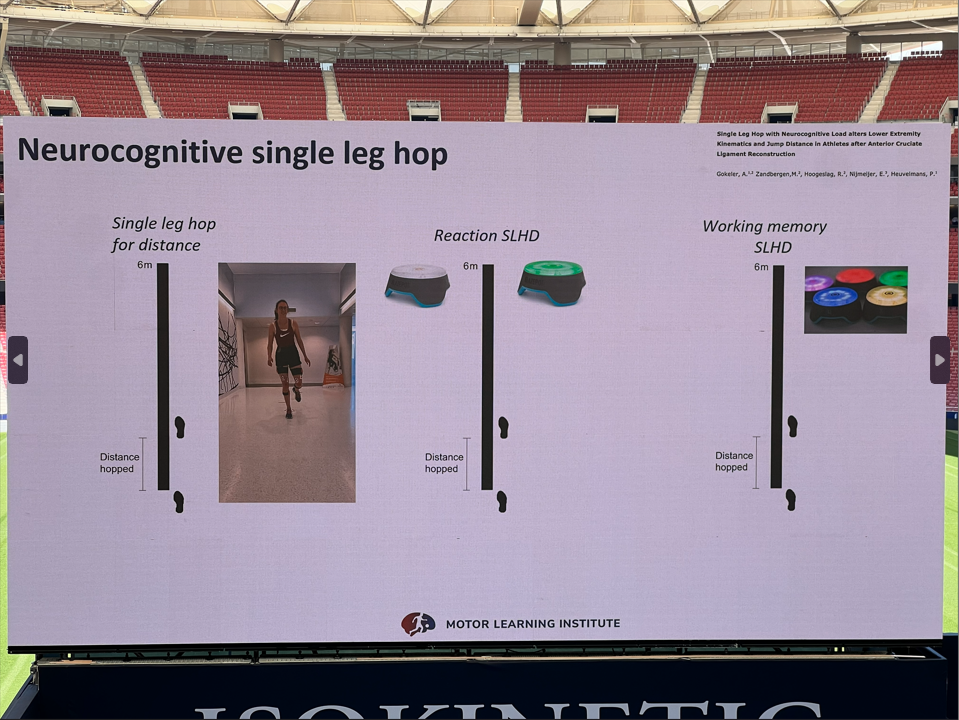
NVM: The simplest way to include this in daily practice is to augment existing functional measures, such as hop tests or agility tests, with neurocognitive challenges. For example:
- Single-leg central hop with stimulus–response reaction.
Instruction: “Jump as far as possible when you see the color red,” while showing the patient different colored cards. - Reactive-memory T-test for agility.
Instruction: “Your activation color is green. In addition, during the test I will show you five colors, remember which ones they are.”
Expensive equipment is not required; this can also be done using simple printed color cards, for example. Creativity is key. When comparing the augmented test with the regular test, a performance difference under dual-task conditions (in hop distance or T-test time) of less than 10% is considered acceptable according to Grooms et al.
AG: And how accurate or representative do you think these tests are in relation to what happens in the real world? Can they help us clinically when prescribing our treatments?
NVM: Of course, we are still refining these tests and they are not fully sport-specific. That is why, as mentioned, creativity is important. Do athletes rely more on vision or on sound during their sport? Try to use the appropriate stimuli so that the test is as sport-specific as possible. And yes, you can also incorporate neurocognitive challenges during the exercises your patients perform in the clinic or on the field.
AG: And now, moving on to the final point regarding psychosocial factors. I remember reading your thesis, in which you mentioned that the first reference to these factors was made by Van Grinsven in 2010. That was, so to speak, only about 15 years ago.
Despite this relatively short time since psychosocial factors were first included, in your editorial you explain that in the most recent guidelines we have discussed, psychosocial factors are only briefly mentioned, limited to pointing out the scales used to measure aspects such as fear of re-injury, psychological readiness, or kinesiophobia: Patient-Reported Outcome Measures (PROMs). Some of the most commonly used in knee rehabilitation include the ACL-RSI, TSK-11, PHOSA-ACLR, K-SES, among others.
And perhaps this translation of science into clinical practice is more common in countries such as the United States, where scales and questionnaires are used routinely, and in others like Spain, through physiotherapists who are more specialized in knee rehabilitation.
However, after reading your editorial, I am the first to reflect on the fact that we are not entirely sure how to interpret these results. We assume that greater psychological readiness or lower levels of kinesiophobia will lead to better outcomes and a lower risk of re-injury, but this is not always the case. Zarzycky (2024) reported that female soccer players with better psychological readiness at return to sport were actually more likely to sustain a re-injury.
And it is true that all clinicians have encountered patients who feel mentally overconfident in contrast to their objective biomechanical measurements. Far from experiencing kinesiophobia, they report no fear and show a strong desire to return to sport. These are the patients we need to slow down, and in reality, they are even more difficult to manage than those who are limited by activity avoidance.
So, what would you say to clinicians is important to consider today, based on the research we currently have, regarding what we should measure in the psychosocial domain and how to interpret those results?
NVM: I believe the most important thing is to be aware of the psychological aspect of an ACL injury or surgery. Patients are dealing with their emotions, they feel fear, they feel alone… talk to them about this.
Questionnaires such as the ACL-RSI or the PHOSA-ACLR can help identify what their main “weakness” is. Discussing these topics with patients provides them with clarity about their own thoughts.
And let us remember that, as physiotherapists, we do not have to solve everything. Sometimes patients need to be referred to a psychologist, ideally a sports psychologist, to help them overcome their fears.
AG: When do you think we should refer patients to psychologists?
NVM: Physiotherapists often have a close relationship with their patients and can address many psychological issues simply by talking with them, or by using visualization exercises or gradual exposure. If all of this does not work and the time to return to sport is approaching, do not hesitate to seek the support of another professional.
There is truly a great deal to reflect on, and we hope we have encouraged the professionals who have accompanied us to do so, in order to improve the care we still need to provide to patients with ACL injuries despite the continuous progress being made.
AG: And regarding everything we have reflected on, you mentioned that the ESSKA group, of which you are a member, will publish a new ACL guideline in 2026. Can you tell us about the work you are doing on this and when it will be published?
NVM: Officially, it is a consensus, and we have been working on it for more than a year. The ACL rehabilitation consensus is being developed by a group of experts, including physiotherapists, researchers, and orthopedic surgeons, from Europe (ESSKA) and the United States (AASPT and AOSSM).
The process begins with a group of experts who formulate clinically relevant questions, covering topics ranging from prevention and early rehabilitation to return to sport. Subsequently, another group of experts conducts literature searches for each of these questions. It is an extremely time-consuming process.
After gathering all the literature, the first group of experts, who formulated the questions, is tasked with drafting the answers, known as statements, based on the evidence and expert opinion. This phase has already been completed.
The next step is to ask another group of independent experts to review and rate all of these statements. The ACL rehabilitation consensus will be finalized at the beginning of this year and will be presented for the first time at the ESSKA Congress in Prague in May 2026. In addition, ESSKA will publish the consensus on its website, where it will be available for free download.

AG: Without a doubt, with this great news about the publication of the new guideline in 2026, we can bring this conversation to a close. Thank you so much, Nicky. Do you have any final thoughts or messages you would like to share?
NVM: Thank you, Ana, and Knee Spain, for this interview. This will be my last one as a researcher and physiotherapist, as a few years ago I decided to focus solely on research, and now I will also be stepping away from this field. From February 2026 onwards, I will no longer be working in the ACL world.
It has been an incredible journey, and I have made so many friends all over the world. Thank you to everyone who has contributed to this crazy adventure. Now it is time for new adventures and for spending more time with my family. But I am sure these friendships will last forever.

AG: Thank you so much, Nicky. For your time on this article, for the opportunity you gave that Spanish physiotherapist interested in the world of the knee to keep opening that path, and, forever, for your friendship.

